OpinionCoronavirus: lockdown, vaccine, herd immunity. Can there be a winning exit strategy?
- There are many unknowns about Covid-19, but one thing is for sure: every possible way out is riddled with hard choices
- Here are four graphs that explain why

For millennia, many Native American tribes used fire to fight fire by starting small controlled forest fires to clear away undergrowth and debris. Without controlled fires, combustible material accumulates over time until a stray spark starts an unstoppable fire fuelled by all the accumulated debris.
Lockdowns buy precious time but are not a strategy. The immediate fire is extinguished but the population remains vulnerable as large numbers lack any immunity to Covid-19 – akin to a forest-full of combustible material. It will only take a spark.
Exit strategies for Covid-19 must consider this longer perspective, but the following charts explain why there will be no easy solutions and many ethical dilemmas lie ahead.
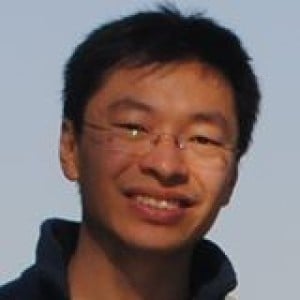
CHART 1: POPULATIONS ‘EXIT’ COVID-19 ONLY WHEN HERD IMMUNITY IS ATTAINED
